
Shoulder dislocation is more common in the younger and more athletic population. To prevent and treat shoulder dislocations you need to improve the shoulder’s stability – which is provided through the ligaments and muscles.
For further information the muscles of the shoulder and rotator cuff have been discussed in the previous Blog.
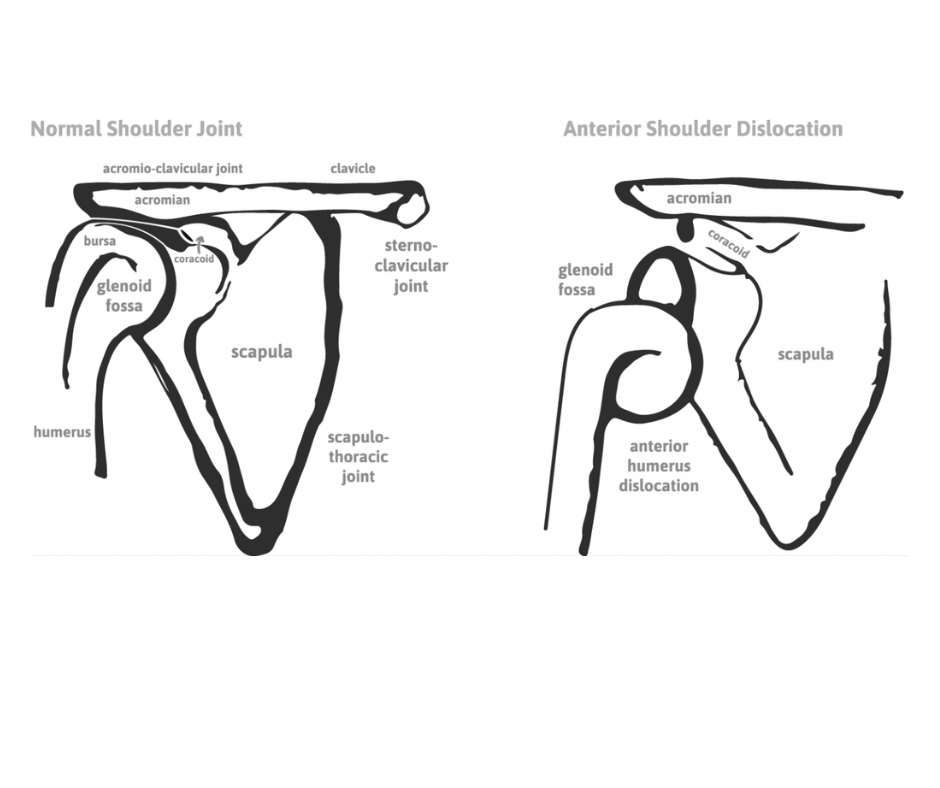
The shoulder can dislocate towards the front (anteriorly), to the back (posteriorly) or downwards (inferiorly). It is more susceptible for the shoulder to move anteriorly – 95% of shoulder dislocations are anterior compared to 3% posterior and 2% inferior. This is due to the anatomical features of the glenoid fossa. The cupped shaped part of the scapula where the head of the humerus sits. It is not the full size of the humeral head.
The advantage of this is the full circumduction movement of the shoulder – so we can perform a lot of activities. However, the disadvantage is that the shoulder is not as stable. There is a glenoid labrum is soft tissue – ligament like structure – which extends the edges of the glenoid fossa to make it a larger surface area. A full shoulder dislocation is where the humeral head fully comes out of the glenoid fossa. A subluxation is where the humeral head only partially moves out of the glenoid fossa.
Most dislocations are a result of trauma; however, a few people have congenital dislocation so abnormal muscle or collagen control around the shoulder. The shoulder is at it’s weakest position in 90 degrees abduction with full external rotation. Sports where throwing from this position regularly are at higher risk of these injuries. For example: water polo, baseball, and volleyball.
If the shoulder has dislocated then approximately seven out of ten people will dislocate their shoulder again. This recurrence is much more common in adolescents.
How to Assess Shoulder Stability?
To assess your shoulder stability, the shoulder stability index gives a patient directed effective assessment to determine baseline and improvements of shoulder stability
Exercises to improve stability:
At The Hands Physio your hand therapist will give you these exercises in the form of a YouTube video for easy reference and to ensure correct application of exercises. It is important to have a professional lead you through these exercises if recovering from an injury.
As your ligaments have been disrupted with a shoulder dislocation, your ability to know and respond to where your arm is in space – your proprioception – will be disturbed as well. You will also need to do exercises to restore this as well.