
Shoulders are broad not only physically but metaphorically too. While we stand on the shoulders of those who have gone before us, we also carry the weight of the next generation upon our own shoulders!
Our shoulders affect our posture and our posture not only matters to prevent injury but also signifies how we present to the world. To stand tall, with your shoulders back this is to embrace who you are and what is ahead with strength and confidence.
Therefore, it is critical our shoulders are strong and the musculature remains balanced. The muscles of the shoulder are extremely important and significant in the movement of the upper Limb.
There are three bones of the shoulder. The clavicle, the scapular, and the humerus. The sternum and the thoracic wall are also in close proximity to and necessary for the correct functioning of the shoulder. A therapist’s great skill is the ability to palpate the major sources of pain and injury on the surface of the body.

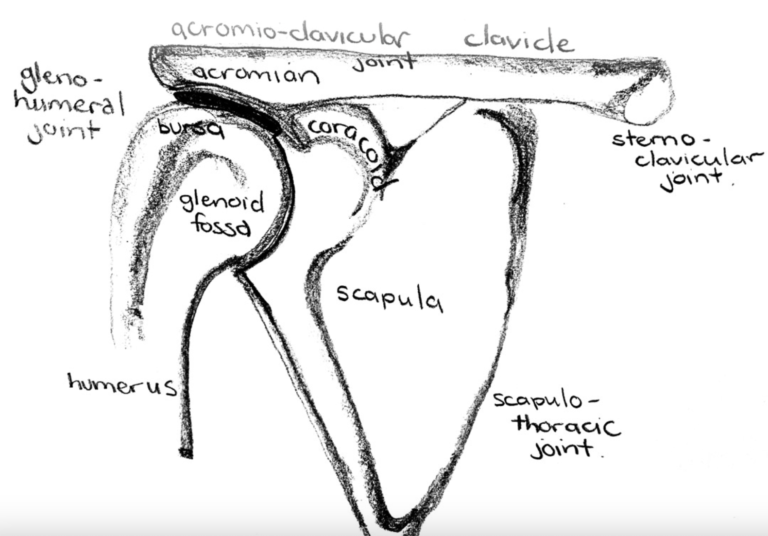
The articulations between these bones creates the four unique joints of the shoulder:
The bursa lies under the acromion to cushioning and shock absorption to the supraspinatus muscle. Gliding surface.
The large muscles of the shoulder, neck and thoracic wall are:
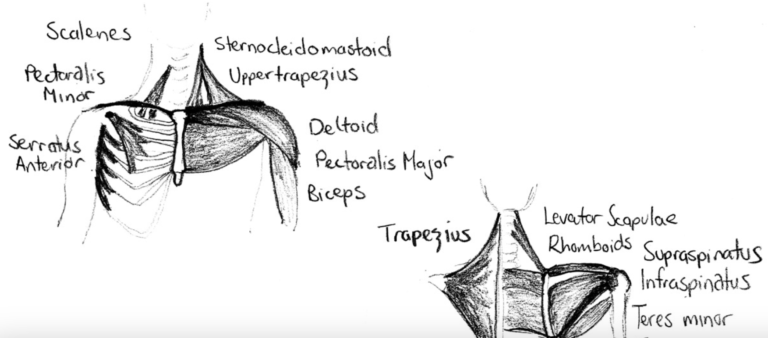
There are four rotator cuff muscles of the shoulder. These muscles are responsible for the correct motion of the shoulder. They ensure that the head of the humerus stays positioned squarely and tightly in the glenoid fossa of the scapular:
The supraspinatus and the infraspinatus are supplied by the suprascapular nerve (nerve root C5/6) which runs through the small suprascapular notch in the scapular – so this is an area for impingement. Weakness in abduction and external rotation. It is important to clear the nerve roots C5and C6 in the neck as they supply all the muscles in the shoulder region.
These muscles together work to hold the head of the humerus in the centre of the glenoid fossa throughout the full movement of the arm – from by your side to up overhead – and are tested with palpation and then resist the movement of the muscle.
Injuries to the tendons and muscles of the shoulder are usually a result of:
When muscles are operating in shortened positions, they are inefficient in using energy. Therefore, in simple terms, it takes more energy to do the same movement, consequently, the muscles get tighter and more acid builds up.
Nerves are superficial and run along some very tight spaces in between some small spots, so nerve traction and compression are common sources of injury. The bones themselves degenerate naturally so spurs, osteophytes & nodules develop. This then puts pressure on to the tendons. Repetitive overuse of the shoulder with underlying poor mechanics commonly leads to impingement injuries.
Forces of the Rotator cuff
The deltoid and supraspinatus both contribute to the abduction of the arm. The resultant force of both muscles is a compressive force holding the humeral head in the glenoid fossa as the arm moves overhead.

The infraspinatus & terres minor externally rotates the arm and the subscapular is internally rotates the arm. The coupling action of these muscles adds a compressive force towards the glenoid fossa as well providing additional stability to the joint. The combined action of these muscles holds the humeral head in the glenoid fossa as the arm moves in all positions. Balance of these muscles prevents impingement of the tendons.
All four muscles of the rotator cuff join together when they insert on the humerus, so act together rather than in isolation. The change invascularity of the supraspinatus tendon as we age is still under debate. Cadaver studies have shown a hypovascular area within the critical zone of the supraspinatus tendon, while patients with supraspinatus impingement have demonstrated hypervascularity due to injury from mechanical impingement
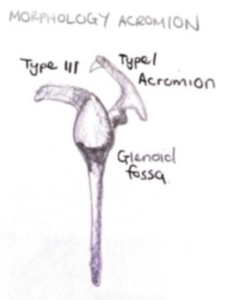
Patients with a Type III Acromion – where the acromion hooks around further compressing the supraspinatus tendon – tend to have a higher prevalence of rotator cuff tears compared to the Type I and II Acromion positions that are more rounded and provide more space naturally.
Imbalance and Weakness of the Rotator Cuff Muscles
Repetition of movements, especially overhead, greater than 60 degrees abduction/flexion can lead to rotator cuff tendon tears. Stress on the tendon is similar either side of the acromion and bursa.
Acromial Spurs
The presence of acromial spurs, as a result of arthritis, is a factor present in supraspinatus tendon tears, in the older population.
Tendon Morphology
Intrinsic changes within the tendons making them susceptible to the development of tears. The rotator cuff tendons tend to degenerate with age.
Internal Impingement
Internal impingement occurs when the cuff is pinched between the humeral head and the posterosuperior labrum during extreme abduction and external rotation. This scuffs and abrades the articular surface of the cuff progressively leading to cuff tears especially in overhead athletes.